Painkillers, Heroin and Addiction: The Opiate Crisis Laid Bare
From East to West, North to South, the Opiate addiction continues, almost unchecked, to claim lives, destroy families and ruin communities.
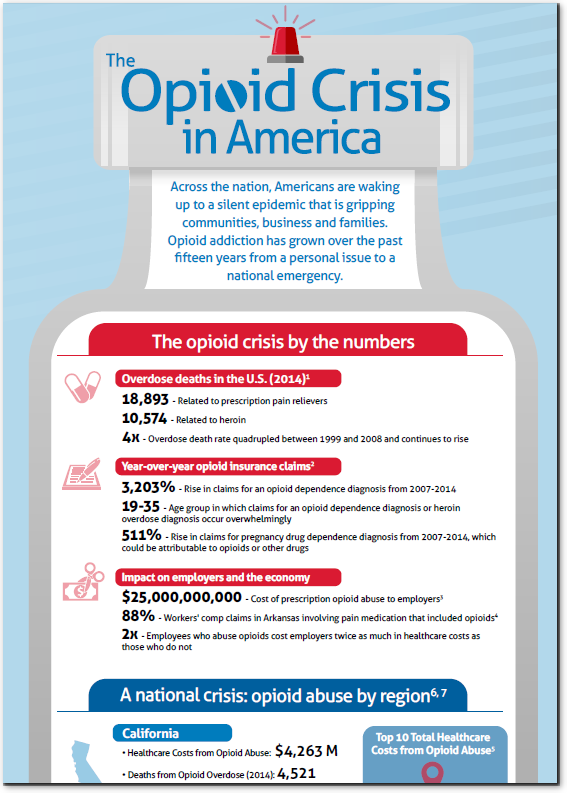
Opiate Addiction: The Overdose Emergency
Fueled by both prescription painkillers and illegal substances, opiate addiction kills thousands every year. In 2014, for example:
Despite those shocking numbers, the problem continues to grow. (It quadrupled in the first decade of this century and continues to explode). In the past twelve months, the Drug Enforcement Agency (DEA) has been forced to issue warnings on new drugs such as Fentanyl, a potent opiate more than 100 times more powerful than morphine and 30-50 times stronger than heroin. While Fentanyl has killed thousands of people over the past few years, many only heard of it recently, when it was attributed to the death of the musician Prince.
Still, by far the most prevalent cause of overdose is prescription painkillers. This encompasses a much broader swath of the Opioid family (Opiates and their synthetic and semi-synthetic variants). The most common culprits are:
In 2014, the United States saw nearly 4.3 million people ages 12 or older using prescription painkillers non-medically. To put that into perspective, that is almost 2% of the entire population. According to the Centers for Disease Control, more than 1,000 people are treated in emergency departments for misusing prescription opioids every day. Finally, almost 2 million Americans either abused or were dependent on prescription opioids in 2014.
Painkillers, Addiction and the Economy: What the Opiate Crisis is Costing America
The opiate addiction crisis has an obvious and tragic human cost. Addiction to painkillers and illegal opiates cause death and healthcare emergencies every day. But they also have a profound economic cost that affects people, employers and governments all over the country.
One estimate, conducted in 2011, put the economic cost at $55.7 billion
Of those figures, the study’s authors offered the following breakdown:
To put that in perspective, the $55.7 billion that opiate addiction erases from the economy is roughly equivalent to the annual Gross Domestic Product of the entire state of Maine. It is greater than that of Alaska, North Dakota, Montana, South Dakota, Wyoming and Vermont.
Medication, Therapy and Shifting Thinking: Opiate Addiction Solutions
Opiate addiction is deadly, it’s costly, but it is anything but simple; especially when it comes to finding solutions or even identifying the root causes of this crisis. Some point to the high availability of opiates compared to the past — the number of prescriptions for opioids (like hydrocodone and oxycodone products) escalated from around 76 million in 1991 to nearly 207 million in 2013 — others point to socioeconomic factors or to the increased focus on pain management in recent decades.
The answer is, most likely, that all of these answers are correct, at least some of the time. Tackling opiate addiction and prescription painkiller abuse will take a multi-faceted approach which recognizes that while opiate addiction and overdoses are the hurdles, there are many different paths to overcoming them.
One such solution is increasing the availability of medication-based treatments for opiate addiction. Both Medication Assisted Treatment (MAT) and Office Based Opioid Treatment (OBOT) offer physician-supervised treatment options that use several medications to treat and even prevent addiction to opioid painkillers. These treatments combine medication with behavioral therapy to help ease a patient away from their opioid addiction over time and have been proven to be highly effective. However, both MAT and OBOT have obstacles to overcome before becoming more widely accepted for use.
There are challenges matching medication providers with supportive counselors as well as a lack of access to prescribing physicians. Furthermore, there is some opposition to MAT and OBOT from providers that support 12-step programs as well as among providers who view such methods as swapping one addiction for another. Both MAT and OBOT have been clinically proven to be an effective tool for overcoming addiction to both prescription painkillers and illegal analogs such as heroin as well as alcohol.
A second option for solving the opiate addiction crisis is to change techniques for pain management entirely. For example, back pain is one of the most common reasons Americans go to the doctor. From 2001 to 2011, the number of spinal fusions in U.S. hospitals increased 70 percent, making them more frequently performed than even hip replacements.
This reliance on surgery is controversial. Although many patients expressed satisfaction with the outcome of surgery, 51% of patients who were using opioids before the surgery still were using the drugs one year later, and among those who were not using the drugs before surgery, 18% were using them a year after their surgery.
An increasingly popular alternative is to channel more people, where appropriate, away from opioids and surgery and into more effective treatments such as physical-therapy. By reducing the number of people being introduced to opiate painkillers, the number of people who develop an addiction is reduced.
Thirdly, there is increased interest in deploying Cognitive Behavioral Therapy (CBT) to improve treatment response as a primary or conjunctive treatment option. CBT is a particularly appealing solution for some as it can be deployed in very innovative ways, both in-person and online and it remains just as effective. CBT can help people with an opiate addiction by teaching the patient to recognize and avoid negative and destructive thought patterns and behaviors. This teaches the individual to recognize the triggers that cause a craving for drugs, then avoid or manage those triggers. CBT works well in conjunction with other treatments.
Other non-opiate based interventions for pain include mindfulness therapy, the use of non-addicting medications such as non-steroidal anti-inflammatory agents (NSAIDS) and anti-depressants to name a few.
A Pioneer in Substance Use Management
Magellan Health is a pioneer in offering integrated, comprehensive opioid risk and substance use management programs. We have an unyielding commitment to ending the current epidemic. And we are uniquely positioned to bring together behavioral, medical and pharmaceutical programs to positively impact overall population health and reduce cost.
We offer many substance use solutions, including medication assisted treatment (MAT), shown in the monograph as an invaluable tool in the fight against substance abuse. We continue to evolve our MAT program and other offerings to most effectively meet the needs of our customers and those they serve.
 Dr. Shareh Ghani, vice president medical director at Magellan Healthcare, and lead author of the study spoke of the importance of fully understanding the scope of the addiction crisis: “Having worked in commercial and Medicaid markets, I have reviewed numerous cases of accidental overdose and suicides related to pain prescriptions. The opioid crisis in this country demands that we understand the issue and identify predictors of risk.”
Dr. Shareh Ghani, vice president medical director at Magellan Healthcare, and lead author of the study spoke of the importance of fully understanding the scope of the addiction crisis: “Having worked in commercial and Medicaid markets, I have reviewed numerous cases of accidental overdose and suicides related to pain prescriptions. The opioid crisis in this country demands that we understand the issue and identify predictors of risk.”